
Watery Eyes Frequently Asked Questions – London
What causes a watery eye?
A watery eye can be due to many causes. It is essentially an imbalance between the amount of tears being produced by the tear gland and amount that can be removed by evaporation and the tear drainage system. Problems with the eyelid or narrowing of the drainage canals can prevent tears being drained into the nose. Some people have more than one factor causing their watering. Even some people with dry eyes may also experience watering due to reflex tearing as the eye attempts to keep itself moist.
What is a blocked tear duct?
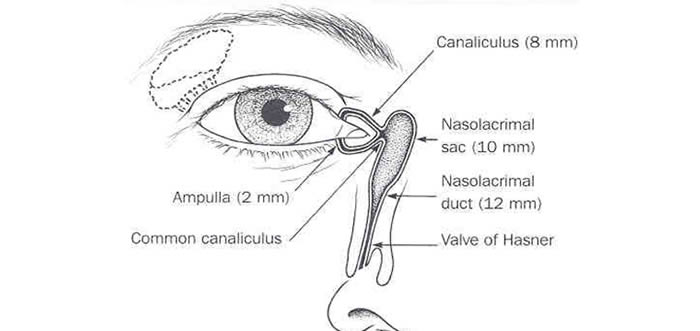
Tears are produced continuously and are drawn into a small hole in the inner corner of your eyelid known as a punctum. There is one in the upper and lower eyelid. They lead into small tubes known as the canaliculi, which in turn drain into the lacrimal or tear sac. This lies between the corner of your eye and your nose and has a duct at the bottom, which drains into your nose, the nasolacrimal duct. If the nasolacrimal duct blocks the eye becomes watery, and sometimes sticky. Some people develop a painless swelling of the tear sac at the inner corner of the eye and a few get repeated painful infections, like a boil or abscess.
Why does blocked tear duct occur?
The normal tear drainage system does not have much spare capacity, which is why the tears spill onto your face when you produce excessive tears such as when you cry. The narrow drainage channel becomes even narrower with age, especially if there has been nose or sinus disease.
How do I know if I need an operation?
Your doctor will examine you to see if your watering is due to a problem in the tear drainage system. This will include syringing water through the tear ducts to see whether there is a blockage. A endoscope/telescopic is used to examine the inside of your nose. Sometimes a x-ray examination of the tear drainage pathway (a dacryocystogram or dacryoscintillogram) is needed to help determine the cause of your watery eye or the site of obstruction to tear flow.
What does the surgery involve?
The surgery creates a new pathway between the tear sac and the inside of the nose by removing a small piece of bone between them and bypassing the blocked nasolacrimal duct. This operation is called a dacryocystorhinostomy or DCR for short.
The operation is performed in one of two ways:
- The endonasal approach avoids a skin incision and is performed through the nose using an endoscope.
- If the nasal passage is too narrow the external approach is used, through a 1.5cm skin incision on the side of your nose, where a pair of glasses would rest. This heals up very quickly and in most people is nearly invisible when healing is complete. There will be a stitch, which will usually be removed seven to ten days after the operation.
The success rate of the approaches through the nose and through the skin are the same. Your doctor will tell you which approach is most suitable for you.
In a few patients, a small soft silicone tube or stent is placed in the tear duct/canals to keep the passages open while healing takes place. This is removed 6 weeks after the surgery in the outpatient clinic.
How successful is the surgery?
In most cases where the obstruction of the tear duct is in the nose, there is a 90-95% success rate. This means 1 in 10 people may not improve after surgery.
Rarely if the obstruction is in the tiny tear canals on the eyelid (canaliculi), the success rate is less and can vary between 50-90% depending on the exact site and extent of blockage.
What type of anesthetic is necessary?
The operation takes about an hour and is usually performed under a general anesthetic where you are asleep, or under local anesthetic with intravenous sedation to make you sleepy so you do not feel any discomfort.
You may be able to have the surgery as a day patient and go home the same day or you may be admitted overnight. Your doctor will discuss which will suit you best at your consultation.
What should I do in preparation for surgery?
Blood thinning medications such as aspirin, clopidrogel (Plavix, Iscover) and warfarin can make bleeding more likely and severe during and after surgery. If you are taking these drugs we may need to ask your GP or cardiologist if and when to stop these medications prior to surgery. You should also stop anti-inflammatory drugs like ibuprofen (Nurofen), fish oil, ginger, ginseng and garlic containing supplements 2 weeks before surgery.
Is there anything I should not do after the operation?
After your operation, plan to rest and avoid strenuous exercise, running or heavy lifting for a week. You cannot drive, operate machinery, drink alcohol or take sedative drugs for 24 hours. Do not blow your nose for 2 weeks and avoid very hot food and drink for 2 days after the operation as these can increase the risk of bleeding. Most people require a week off work.
What happens after surgery?
After the operation you may have some blood/pinkish discharge ooze from the nose. This usually stops within a few days. There is usually no significant pain after the surgery. You may note some aching, tenderness, swelling and bruising on the side of the nose and around the eye. You will be given a saline nasal spray which you should spray up the nostril on the side of the surgery twice a day for 2 weeks to wash away any old blood and discharge from the nose. Do not travel on an airplane for 2 weeks after surgery.
What is the follow-up treatment?
You will be given a clinic appointment for 7-10 days after surgery. If you have had a stent inserted at the time of surgery, they may be just visible in the corner of the eye between the two eyelids. This will be removed at your outpatients appointment 6 weeks after surgery.
What are the main complications following a DCR?
Bleeding: A nose-bleed can occur up to 14 days after surgery. This happens to about 1 in 100 patients. In most cases the bleeding will stop by itself or with icepacks, but if it continues or is very heavy you should attend the accident and emergency department at your nearest hospital.
Infection: Infection of the wound or sinuses may rarely occur in 1 in a 100 people usually within the first week and is treated with oral antibiotics. If you develop a temperature or increased nasal or facial pain then seek medical advice.
Failure of the watery eye to improve: This occurs in 1 in 10 people and can sometimes be improved with a second operation.
Contact us to learn more about Watery Eyes (Dacryocystorhinostomy)
